How effective are 'non-medical interventions' that reduce human-to-human contact in preventing pandemics?

Influenza and other infectious diseases are spread through human-to-human contact.To prevent the spread of the new coronavirus (SARS-CoV-2), remote work is recommended around the world, schools are Has been closed. Such people and was aimed at reducing the contact with people 'non-pharmaceutical interventions (NPI)' is an essential element for mitigating the spread of infectious diseases, 'all over the world to the 1918
Public health interventions and epidemic intensity during the 1918 influenza pandemic | PNAS
https://www.pnas.org/content/104/18/7582
A study published in 2007 by Richard J. Hackett and colleagues examined the impact of public health interventions by cities in the United States on the 1918 Spanish cold. At the time of the 1918, NPI was implemented in the United States in 17 cities and 19 districts at different times for the Spanish cold. The research team obtained data from that time and looked at 'how much does early NPI impact prevent infectious disease spread?'
The reason why we measured the effects of NPI instead of antiviral drugs and vaccines is that in the early stages of a pandemic, antiviral drugs and vaccines are often not widely available.

At that time, the NPI implemented in the United States was different in type and timing implemented for each city. Many cities have closed schools, churches, theaters, dance halls and other public facilities. The NPIs actually implemented and the number of cities that implemented each measure are as follows.
・ Spanish cold (flu) can be notified (15 cities)
・ Announce emergency (4 cities)
・ Separation policy (14 cities)
・ School closed (14 cities)
・ Close church (15 cities)
・ Closed theaters (15 cities)
・ Dance hall closed (11 cities)
・ Close other facilities (13 cities)
Shift business hours to reduce congestion in commercial stores and transportation (8 cities)
・ Announce mask ordinance (2 cities)
・ Prohibit tram congestion (6 cities)
・ Private funeral (11 cities)
・ Prohibition of door-to-door sales (1 city)
・ Interventions to reduce workplace infections (0 cities)
・ Protective isolation of children (3 cities)
・ Prohibition of public meetings (15 cities)
・ Prohibition of congestion in places other than transportation (3 cities)
・ Close business in the entire community (1 city)
Research has shown that cities with multiple NPIs in the early stages of the Spanish cold epidemic have about 50% lower peak mortality than other regions. It has also been shown that the rate of excess mortality is about 20% lower in areas where NPI was implemented early than in others, but there was no statistically significant difference in this figure. That is.
The chart below summarizes the mortality rate (number of deaths per 100,000) from Spanish cold in Philadelphia (black line) and St. Louis (dotted line). The first case of a Spanish cold in Philadelphia was reported on September 17, 1918, but authorities disregarded its importance, and a large-scale citizen rally took place on September 28 of the same year . The NPI, which closed schools and banned large-scale gatherings, was not implemented until October 3 of that year. In contrast, the first case in St. Louis was reported on October 5, 1918, and on October 7, two days later, an extensive NPI was implemented to reduce human-to-human contact.
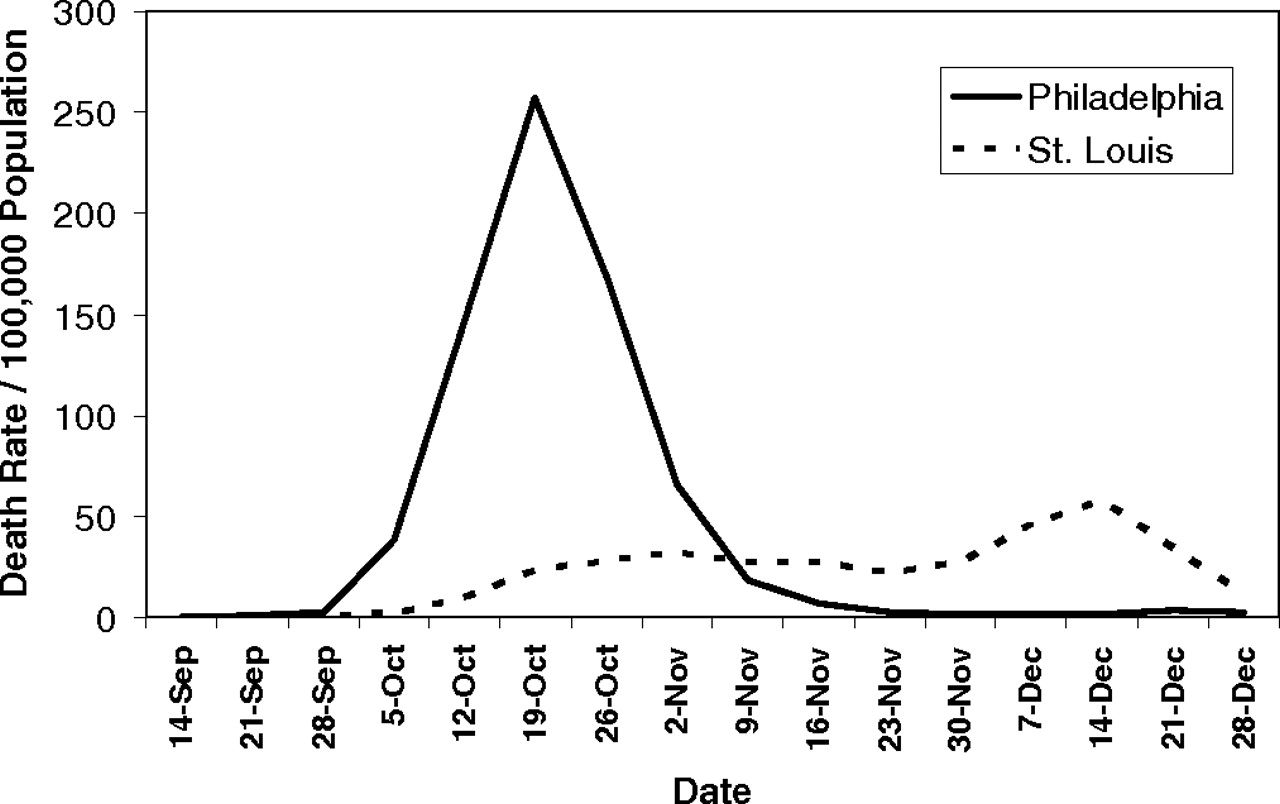
As a result, as can be seen from the graph above, the mortality rate is greatly different between St. Louis and Philadelphia, with the peak mortality rate exceeding 2.5 million in Philadelphia, but exceeding 50 in St. Louis It is suppressed by the degree. The epidemic of the Spanish cold in Philadelphia is three to five times higher than in St. Louis, and the delay in the NPI implementation is 'significant', the researchers noted.
A survey of the Spanish common cold in Philadelphia between September 8 and December 28, 1918 found that mortality from pneumonia or influenza was 257 / 100,000. In contrast, the mortality rate from the common cold in St. Louis in the same period was 31 out of 100,000, less than one-eighth.
Related Posts:






in Science, Posted by logu_ii